Lipomas are common subcutaneous (under the skin) benign (non-dangerous) tumors, which comprises of fat cells. They are for the most part delicate to the touch and movable.

If you try and touch the lipomas, it will feel like a small rubbery, spongy ball, and you would be able to even move it around with a finger. They are in capsule form (encapsulated), and do not spread to the tissues around them.
Clinically, lipomas are often present specifically in the head, neck, shoulders, and backs of patients. However, they can less commonly be seen elsewhere, for example, the thighs. Less commonly, they can also be found on internal organs, such as the stomach and bowels.
The masses are often benign, and while the age of onset can vary. There is usually no reason for treatment. They pose no threat to the patient unless they are uncomfortable due to being located on joints or rapidly growing, which is uncommon, as the typical lipoma growth is slow. If lipomas are not painful and harmless, there is no need for removal.
Patients often complain of a soft, mobile mass of tissue they can feel under the skin. These are typically painless unless they encroach joints, nerves, or blood vessels. Patients often see these in the upper part of the body. Rarely, these lipomas can form in muscles or organs. These masses are typically less than 2 inches wide but maybe larger. They are commonly singular. However, some patients have more than one.
While the age of onset for a lipoma varies, it is typically first seen in patients between the ages of 40 to 60. Certain types of lipomas are more frequently seen in other age groups. For example, such as hibernomas clinically present around the age of 30, lipoblastomas, and diffuse lipomatosis are commonly found in children older than the age of 3. Approximately 5% of patients present with multiple lipomas.
The prevalence of lipomas has been cited as affecting 1% of the population, while its incidence, which is possibly underreported, is 2.1 per 1000 individuals per year.
CAUSES OF LIPOMA
While the etiology of lipomas is unclear, some studies have shown a genetic link, whereby about two-thirds of lipomas demonstrate genetic abnormalities. In addition to the possibility of a genetic link, another theory presents the idea that there is a direct positive correlation between trauma to an area and lipoma production. In addition to the risk factors listed above, other possible connections that may lead to lipomas are obesity, alcohol abuse, liver disease, as well as glucose intolerance.
Lipomas can sometimes, though rare, be associated with certain disorders such as multiple hereditary lipomatosis, Gardner syndrome, adiposis dolorosa, and Madelung disease.
There has been no proven connection between the development of lipomas and any particular occupation or exposure to chemicals or radiation. Some doctors think that lipomas occur more often in inactive people.
Lipomas (and many of the conditions that cause lipomas) are inherited. Since they’re passed down through families, it isn’t possible to prevent them. You can lower your risk of developing Madelung’s disease (a condition that causes lipomas to grow) by limiting the amount of alcohol you drink.
TYPES OF LIPOMAS

While all lipomas are made up of fat, there are subtypes based on the way they appear under the microscope. Some varieties include:
- Conventional lipoma (common, mature white fat)
- Hibernoma (brown fat instead of the usual white fat)
- Fibrolipoma (fat plus fibrous tissue)
- Angiolipoma (fat plus a large amount of blood vessels, painful)
- Adenolipoma (lipomas associated with sweat glands)
- Myelolipoma (fat plus tissue that makes blood cells)
- Spindle cell lipoma (fat with cells that look like rods)
- Pleomorphic lipoma (fat with cells of all different shapes and sizes)
- Atypical lipoma (deeper fat with a larger number of cells)
- Chondroid lipoma (yellow tumours, which occur on women’s legs)
Some conditions cause multiple lipomas to form on the body. Lipoma-causing conditions include:
- Dercum’s disease: This rare disorder causes painful lipomas to grow, most often on the arms, legs and trunk. It’s also called adiposis dolorosa or Anders’ syndrome.
- Gardner syndrome: A form of a disorder called familial adenomatous polyposis (FAP). Gardner syndrome causes lipomas and a range of health problems.
- Hereditary multiple lipomatosis: Also called familial multiple lipomatosis, this disorder is inherited (passed down through families).
- Madelung’s disease: This condition occurs most often in men who drink alcohol excessively. Also called multiple symmetric lipomatosis, Madelung’s disease causes lipomas to grow around the neck and shoulders.
DIAGNOSIS & TREATMENT
Doctors usually diagnose a lipoma during a physical examination. Your doc will touch the lipoma and ask if it’s painful or tender. You may need a biopsy to confirm that the lipoma isn’t cancerous in nature (Liposarcoma). During this procedure, your provider removes a sample of the lipoma and sends it to a lab for testing.

To see a clear picture of this lump, your provider may order an imaging test such as an X-ray, ultrasound, Magnetic Resonance Imaging (MRI) scan, or CT scan.
But, in every case, if you develop lipomas, whether its symptomatic or not, you have to consult your physician. It becomes even more important, if the lipoma is painful, is growing in size over time, is hard to touch, and doesn’t move as easily as normal lipoma does.
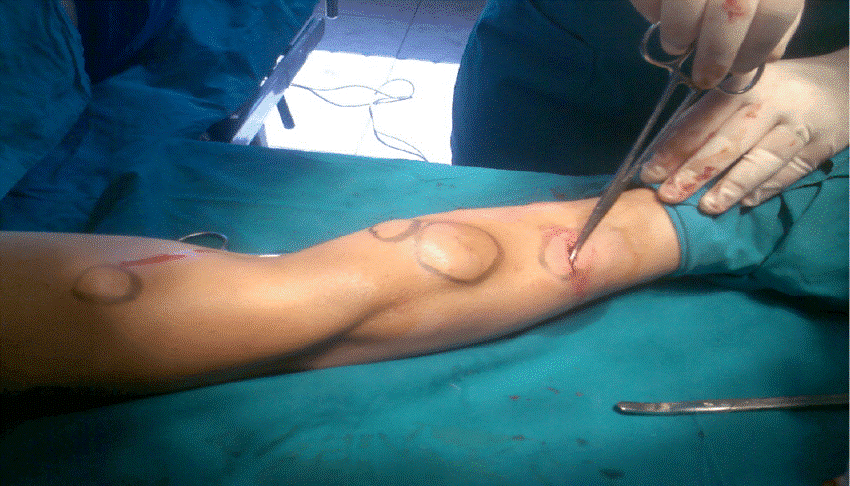
Lipomas are mostly harmless, however, some patients choose to have these masses removed for cosmetic reasons, as they can often be seen through the skin as they lie subcutaneously. Small lipomas (less than 4cm) can be removed through small incisions, and scarring is not usually a significant concern. Open surgery is a better option for removing Giant Lipomas (greater than 10cm) compared with lipoma removal by suction-assisted lipectomy through small incisions as it allows better judgment, prevents recurrences, and avoids damage to the surrounding tissues. Another common method is Liposuction, where you use a needle and a large syringe to suck out the fat from the lump.
The non-surgical options for lipomas include corticosteroids, phosphatidylcholine and sodium deoxycholate injections, all aiming to achieve chemical lipolysis or atrophy of the lesion.
Open surgical excision is the most common intervention with recurrence rate reported to be less than 5% contrary to intramuscular lipomas with recurrence reported as high as 50-80%.
Steroid injections result in local fat atrophy, thus shrinking (or, rarely, eliminating) the lipoma. Injections are best performed on lipomas less than 1 inch in diameter. The steroid is injected into the centre of the lesion; this procedure may be repeated several times at monthly intervals.
Lipomas generally don’t grow back after treatment, but they may grow at any other place on the body, if the person is genetically susceptible.
Most lipomas are best left alone, but rapidly growing or painful lipomas can be treated with a variety of procedures ranging from steroid injections to excision of the tumour.



{kind=link}