The bicycle is approximately 200 years old, believed to have its origins in ancient China, Egypt and India. The past several decades have borne witness to a booming interest in recreational and competitive cycling. Racing, touring and off-road (mountain) bicycles have achieved growing popularity, both as means of transportation, as well as in recreational and competitive athletics.

Cycling is one of the most preferred form of exercising and commuting because, (1) is an uncomplicated form of exercise; (2) is often learned at a young age; (3) is accessible to all ages; (4) can be conducted on an individualized basis; and (5) can be accomplished both indoors and outside (year round).
Bicycling may be the most feasible form of exercise or transportation for individuals due to cost (many sports require extensive financial commitments), physical limitations (injuries may prohibit sports such as tennis, many team sports, or running), or time constraints (commuting may serve as exercise and transportation).
Most significantly, cycling is one of the few forms of physical activity aging populations can do easily with low probability for injury, and thus may increase in prevalence as the population ages.
The increasing participation in cycling and its reported association with erectile dysfunction (ED). Case studies about biking and ED have been reported as early as 1975. Since then, there have been increasing numbers of published reports in the forms of case studies, surveys and clinical investigations, describing a potential cause and effect relationship between bicycling and ED.
Cycling is one of the finest exercises for fat loss, cardiovascular fitness, lower body musculature and overall health. But long hours of cycling can compress the artery and vital nerves leading to the penis.
Bicycle riding’s impact on erectile function remains a topic of great interest given cycling’s popularity as a mode of transportation and exercise. Pelvic pain and numbness are common complaints among male riders. Men with such complaints are more likely to also report ED. Alleviation of factors resulting in pelvic discomfort may reduce cycling’s impact on sexual function.
Let’s discuss in brief about the mail anatomy, which has a link to cycling and ED. When humans sit, they bear their weight on the ischial tuberosities, or what we have come to refer to as the “sit bones.” The ischial tuberosities have no organs attached to them and no nerves or arteries; they are surrounded by the fat and muscle of the buttocks. This area is very well vascularized and allows humans to sit comfortably and safely for hours.
Unfortunately, most bicyclists bear their body weight on a bicycle seat that is not wide enough to support the ischial tuberosities. As a result, they end up sitting on the internal part of their genitals.
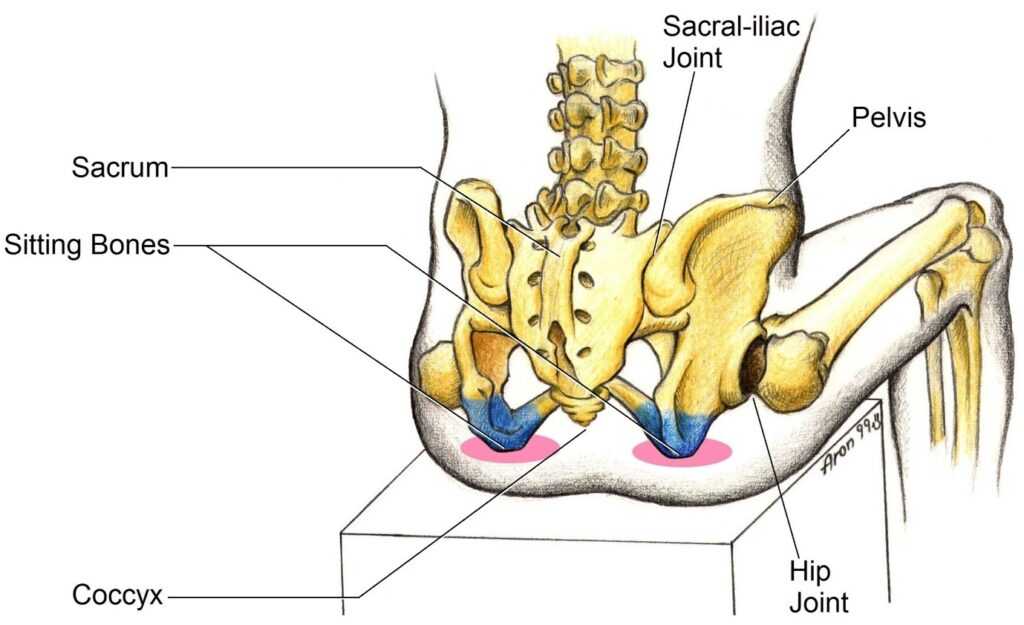
In the straddle position, body weight is supported not by the ischial tuberosities but by the ischiopubic rami, the connector bones that join the ischial tuberosities to the pubic bones. Unlike the ischial tuberosity, which has evolved into the perfect place to bear body weight, the ischiopubic ramus is a working area that contains erectile tissue, nerves, arteries, and the urethra. As a result, the bicycle rider bears his weight directly on an area where the nerves and arteries enter the penis.
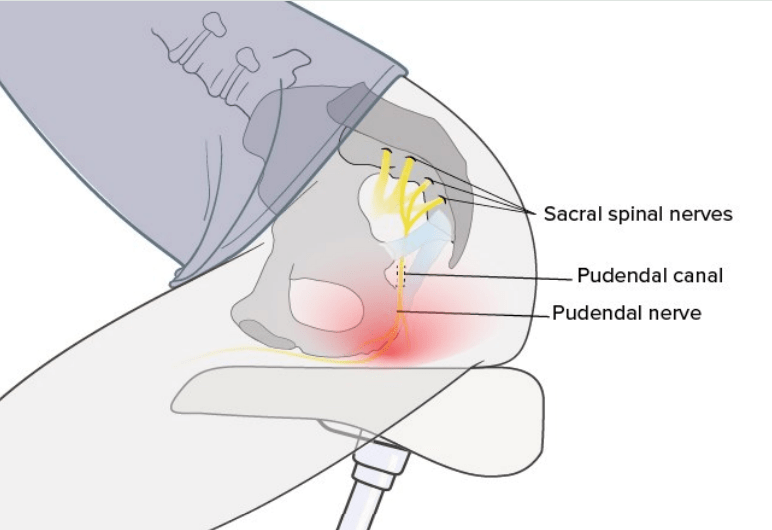
This area is a tube like structure called the pudendal canal, which lies along the ischiopubic ramus. Straddling compresses the nerves and arteries running through this canal against the ischiopubic ramus, which frequently results in complaints of numbness in the penile/scrotal area after cycling. Importantly, straddling may also lead to localized atherosclerosis and compromised blood supply to the penis, resulting in ED.
The pudendal nerve, the main nerve providing sensation of the perineum and controls the pelvic floor, is exposed to frequent pressure and loses ability to sufficiently move when cycling.
Both reduced circulation and increased exposure to compressive forces are proposed as contributors to trauma of the nerve – pudendal nerve compression syndrome. The most recognised symptom is genital numbness, which can be experienced around the perineum, penis, scrotum, or buttocks. Most of the time this is the first symptom of the syndrome and is usually only associated with cycling.
Acc. to a review, several studies have documented a relationship between bicycling and sexual dysfunction. Of the symptoms described, perineal numbness (prevalence of 22–91%) and erectile dysfunction (prevalence of 1.8–50%) are the most commonly reported in the male population.
The primary mechanisms leading to these symptoms in both genders appear to be perineal compression of the pudendal nerve and possible trauma. Rider’s position on the bicycle, as well as different types of bicycle seats, affect the degree of pudendal compression, and consequently the degree of resultant sexual dysfunction.
A study, evaluated risk factors for sexual dysfunction in 1635 male cyclists with the primary intention of determining if genital/pelvic pain and numbness are associated with erectile dysfunction (ED). It was seen that, overall, 22%, 30%, and 57% of men reported ED, genital pain, and genital numbness, respectively. Men reporting penile numbness were at higher risk of reporting ED.
A meta-analysis study, assessed 3,330 cyclists and 1,524 non-cycling controls. Study found a positive correlation between cycling and ED.
A review study, found a significant relationship between cycling-induced perineal compression leading to vascular, endothelial, and neurogenic dysfunction in men and the development of ED. Research on female bicyclists is very limited but indicates the same impairment as in male bicyclists. Preventative measures including use of a properly fitted bicycle, a riding style with a suitable seat position and an appropriate bicycle seat can help prevent impairment of erectile function.
Another review study, found that, bicycle riding more than 3 hours per week was an independent relative risk for moderate to severe ED. The prevalence of moderate to severe ED in bicyclists was 4.2% and 4% vs. age-matched runners 1.1% and swimmers 2%, respectively.
Therefore, bicycle riders should take precautionary measures to minimize the risk of ED associated with bicycle riding: change the bicycle saddle with a protruding nose to a nose-less seat, change the posture to a more upright/reclining position, change the material of the saddle (GEL), and tilt the saddle/seat downwards.
Not all the studies support the notion of cycling leading to sexual dysfunction.
A study, assessed the association of genital numbness and erectile dysfunction in 2,774 male cyclists. Amongst cyclists, there was a statistically significant increase in the trend of genital numbness presence with more years of cycling, more frequent weekly cycling, and longer cycling distance at each ride. Less frequent use of padded shorts and lower handlebar were associated with numbness, but body mass index (BMI) and age were not. Cyclists report genital numbness in proportion with biking intensity but numbness is not associated with worse sexual function.
Another study, examined the associations between regular cycling and urogenital abnormalities in 5,282 men. The data were analysed for risk of self-reported ED, physician-diagnosed infertility, in relation to weekly cycling time, categorized as <3.75, 3.75–5.75, 5.76–8.5, and >8.5 hours/week. Researchers found, no association between cycling time and ED or infertility.

A study, of 125 male cyclists 18 years and over who have had sexual intercourse were compared with 125 men who exercise by running and 125 men who do not exercise. Type of bicycle, type of saddle , cycling position , bike fitting , duration of each cycle and total time from start cycling until now were collected in bicycling group.
Researchers found that, erectile function was significantly higher in cycling and running group when compared with no exercise group. There was no significant differences in orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction in all three groups. No significant differences in all cycling factors on erectile function were found. Thus, both cycling and running can improve sexual health in men in erectile function domain compare with men who do not exercise, and bicycling has no hazardous effect on sexual health in men.
Acc. to an earlier study, the proportion of men with ED is smaller both among moderate or sport cyclists when compared to non-cyclists. Controlling for age, energy expenditure, BMI, smoking and depression, moderate cyclists are less likely to have ED, but sport cyclists appear more likely to have ED.
What the study concluded was something very important. It said that, “elite athletes suffer for their passion. Runners are plagued by joint disorders, football players by knee injuries, tennis players by rotator cuff tears, climbers by torn finger tendons. These athletes compete at a different level than normal individuals. Elite riders are more likely to maintain competition level fitness, join cycling clubs and participate in long distance events. While ED may be a serious concern in an elite population of riders, it must be addressed in this context and should not be generalized to the average cyclist.
In a study, app. 19% of the cyclists tested, who had a weekly training distance of more than 400 km complained of erectile dysfunction. Numbness of the genital region was reported by 61% of the cyclists. The penile blood supply — decreased significantly in over 70% of the test subjects during cycling in a seated position. Cycling in a standing position did not show any alteration in the penile blood supply as compared to the values measured before exercising.
Researchers suggest restricting the training distance, and taking sufficient pauses during the course of prolonged and vigorous bicycle riding, in order to avoid penile numbness and impotence.
A study, assessed the influence of different saddle designs on penile perfusion, in 20 healthy athletic young men (age range 21-31 years) without history of erectile dysfunction. All men were measured in a standing position before cycling, then during cycling in a seated position on a stationary bicycle.
Four different bike saddle designs were used: (A) narrow heavily padded seat; (B) narrow seat with medium padding and a V-shaped groove in the saddle nose (“body geometry”); (C) wide unpadded leather seat; (D) women’s special wide seat with medium padding and no saddle nose.
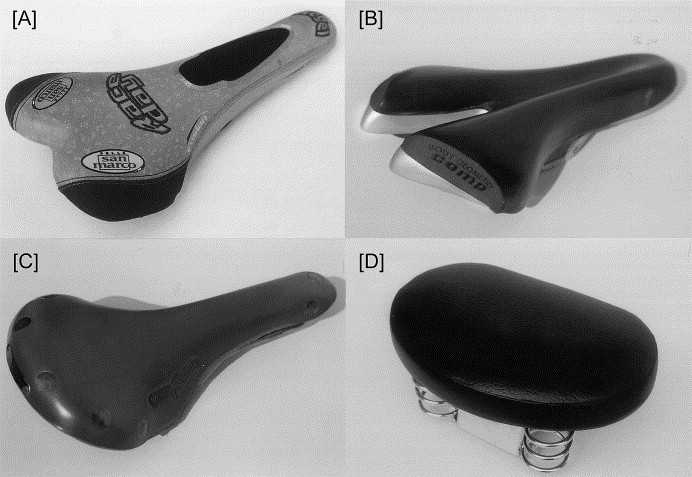
It was seen that, cycling in a seated position leads to a compression of perineal arteries with a consequent significant decrease in penile perfusion. But, there are unexpected differences between different saddle types. The narrow seats and narrow seats with a V-shape in the saddle nose decreased oxygen to penis by 82.4% and 72.4%, respectively.
A study found that, using the no-nose saddle results in a 71% reduction, which was associated with an increase of penile oxygen pressure, reduction of the discomfort in the perineum, and a smaller incidence of perineal numbness. However, this kind of seat was associated with increased posterior seat pressure and greater discomfort in the ischial tuberosities. Additionally, no-nose seats were rated as less stable than conventional seats with a long, protruding nose.
Another study, examined body posture, subjective discomfort, and stability, requiring the participants to ride a stationary bicycle for 20 min, using various combinations of two handle heights and five seat-protruding node lengths (PNLs). The results indicated that bicycle handle height significantly influenced body posture, and that seat PNL caused differences in the riders’ subjective discomfort and stability scores.
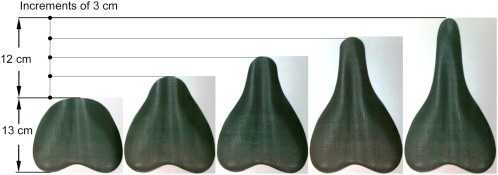
It was seen that, cycling using dropped handles was less stable compared with using straight handles. The results suggested that, a seat with a nose length no longer than 6 cm, would be optimal.
In addition to the type of saddle, the saddle position is also important. The upward tilted seat places greater pressure on the perineum. However, an overly aggressive downward tilt would put undue stress on the shoulders and arms. Cyclists should pay close attention to any early warning symptoms and signs, such as tingling or numbness of the penis. Even in the absence of such symptoms, cyclists should shift cycling positions periodically, rise out of the saddle and take breaks during long rides.
Also, changing your position while cycling can be quite helpful. A study found that, penile blood supply decreased significantly during cycling in a seated position. Cycling in a standing or reclining position (on a reclining bicycle) did not lead to any decrease in penile blood flow. Thus, researchers suggested frequent changes from a seated to a standing position during cycling. Additionally taking sufficient breaks during prolonged and vigorous bike tours, in order to avoid any possible health hazards, was suggested.
Another way to reduce the discomfort and risk of ED would be to adjust the handlebar height, and the type of bike. A study on 463 cyclists found that, cyclists on a long-distance ride may be able to decrease the risk of erectile dysfunction by riding a road bicycle instead of a mountain bicycle, keeping handlebar height lower than saddle height and using a saddle without a cut-out if perineal numbness is experienced.

Acc. to a review study, there are certain good suggestions for cyclists who are worried about ED:
- Cycling should not be discouraged because the cardiovascular benefits are important to both overall and erectile health.
- The cyclist should choose a saddle that allows him/ her to put most or all of their seated weight on their ischial tuberosities.
- A slight tilt downwards of the saddle nose (if present) may help offset some of the anterior compression.
- Make sure the height of the saddle allows for slight flexion of the legs at the lowest point of the pedal.
- The cyclist should try to minimize additional compression between the saddle and the pubic bones. In addition to tilting the saddle, cyclists should make sure that they stand up for at least 15 seconds every 10 minutes of cycling to “rest” the perineum.
- Being an experienced cyclist may be protective, probably due, in part, to a good “fit” and position on the bike. A professional or experienced fitter may be very helpful, especially for the novice or occasional rider.



{kind=link}