To understand maltodextrin, lets understand what are prebiotics. Prebiotics are non-digestible polysaccharides and oligosaccharides that are selectively capable of promoting the growth of beneficial lactic acid producing bacteria in the colon such as bifidobacteria and lactobacillus. A prebiotic is fibre, but not all fibres are prebiotics.
Some of the renown prebiotics include:
- Inulin
- Fructooligosaccharides (FOS)
- Galactooligosaccharides (GOS)
- Trans-galactooligosaccharides (TOS)
- Lactulose
- Polydextrose
- Resistant Starches.
Whereas there are some upcoming prebiotics:
- Hydrocolloids
- Isomaltooligosaccharides (IMO)
- Xylooligosaccharides (XOS)
- Arabinoxylooligosaccharides (AXOS)
- Glucans
- Lactilol
- Raffinose
- Lactulose
- Sorbitol, and…
- Resistant Maltodextrin.
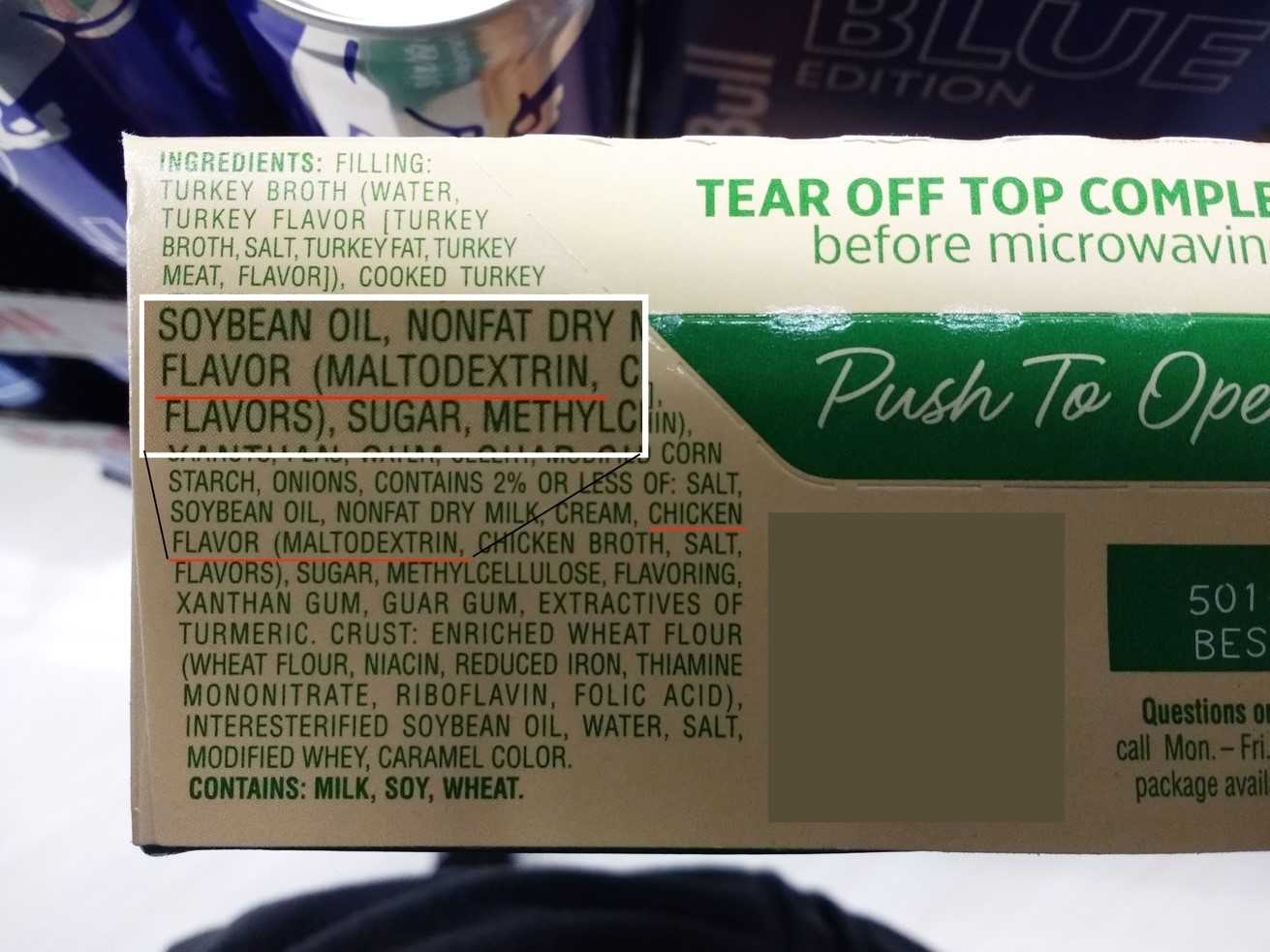
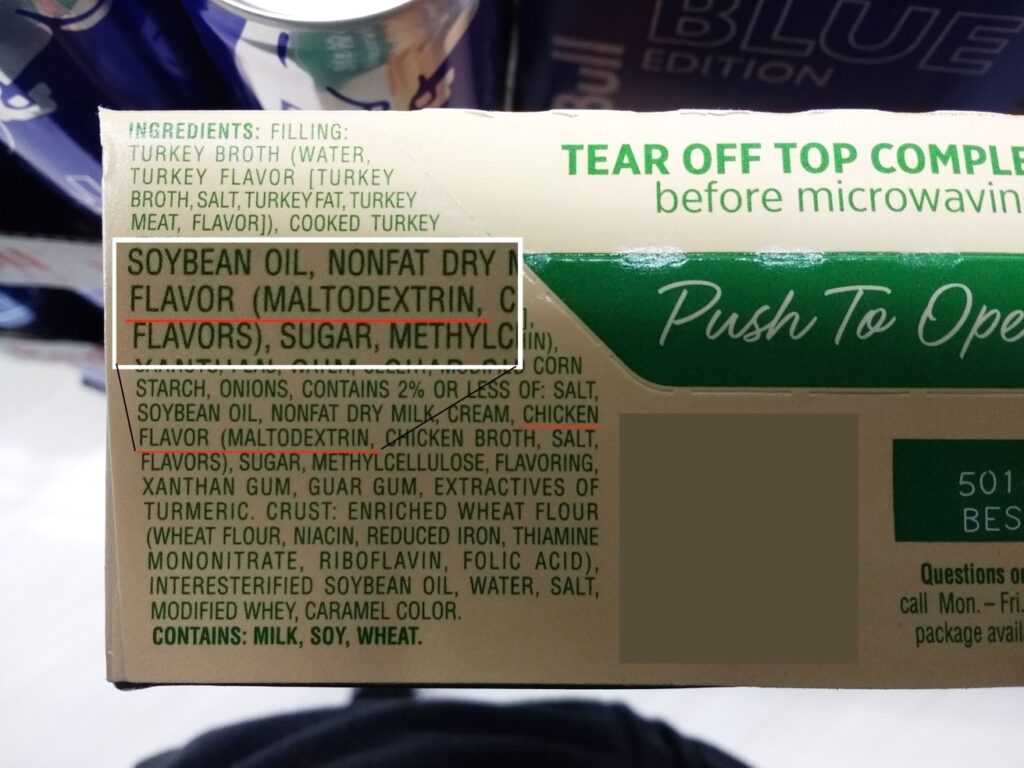
Acc. to a 2016 study, Maltodextrins (MDs) are a class of carbohydrates (CHOs) extracted from a range of sources like wheat, rice, maize/corn, potatoes etc. They are industrially produced by enzymatic or acid hydrolysis of the starch, followed by purification and spray drying. The resulting commercially available, mostly white, powders are of high purity and microbiological safety and are used in a wide range of food and beverage products, including baked goods and sports drinks.

Although confusing to the average consumer, both digestible and resistant-to-digestion type of MDs are commercially used as food ingredients. Resistant maltodextrin that is a compound that is resistant to digestion and degradation by human enzymes.
With an energy value of approximately 4 kcal/g, as underlined by international food law standards, digestible MDs used in foods and beverages have long been considered to be a good source of energy. MDs have found numerous applications in the food, beverage, dietetic, and medical food products, as well as in the pharmaceutical industry in tablet and powder applications.
In recent years, concerns have been raised about the increased use of refined CHOs, including isolated starches and MDs, in food and beverage and its relation to increased obesity rates. One of the main reasons for concern is that, depending on the quantity consumed, refined CHO sources can have a strong impact on the post-ingestion blood glucose, insulin, and lipid levels. Discernible changes in these markers have been linked to potential health risks, especially in vulnerable individuals such as diabetic patients.
MDs are considered to be a good source of energy since glucose obtained from its digestion is readily absorbed in the small intestine and subsequently used in metabolism. The digestion of MDs require same enzymes as the digestion of starch.
It is often suggested that there are differences in the rate of digestion and absorption of MDs compared to glucose. While glucose will be immediately available for absorption upon arrival in the small intestine, MDs have a different digestion process.
The digestion of starch and MDs starts in the mouth by salivary amylase. This enzyme has the ability to breakdown MDs into maltose, a disaccharide consisting of two-linked glucose units. It appears that salivary amylase plays a rather small role in the MD breakdown due to the relatively short time that MDs reside in the mouth. Subsequent to arrival in the stomach, the gastric contents need to be transferred into the small intestinal for digestion and further transit in the gut.
Pancreatic amylase, secreted in the small intestine, plays a final role in hydrolyzing the MDs, a process that leads to the formation of maltose units. Maltose is either taken up by the gut directly or further broken down into free glucose. The obtained free glucose is then transported into the blood. Due to the difference in digestion and absorption, when compared to glucose, it has often been suggested that MDs, as complex CHOs, will require more time for digestion and absorption, resulting in a lower glycaemic response.
This suggestion, however, is a misconception and is not supported by any research data. In contrast, the enzymic digestion of MDs appears to take place at a high rate leading to an absorption rate not being different from absorption after ingestion of pure glucose, as reflected also by comparable post- ingestive insulin responses at rest and during exercise, as well as oxidation rates during exercise.
During absorption, as usual the glucose may be taken up by liver, muscle, brain, and red blood cells, to serve as energy source. The non-metabolized part of glucose will either be stored as liver and muscle glycogen under the influence of insulin.
Although no causal relationship between the consumption of small amount of MDs and negative health effects has been reported, this does not mean that overconsumption of foods containing MDs will have no effect. The regular intake of calorie dense, low-fibre/protein foods or drinks with high levels of refined added carbs, in particular soft drinks and sweet snacks, may easily induce a persistent positive energy balance resulting in weight gain, impaired insulin sensitivity as well as increased blood cholesterol and blood lipids.
One of the most common uses of maltodextrin is in baby foods. There is a strong nutritional reliance on lactose as a source of energy in early human development, preferably as part of the mother’s breast milk. However, lactase deficiency resulting in the inability to digest may lead to malabsorption-induced diarrhoea in which approximately 40% of the energy provided may be lost. In such cases, MDs can be used as a substitute for lactose to provide energy.
In this respect, it is suggested also that the use of MDs, instead of glucose is favourable since this helps reduce osmotic load and related intestinal distress. MDs are also used as a carb source in nonallergic infant formulae containing non-dairy proteins (soy). Moreover, maltodextrins are suitable for infant nutrition as they are easy to use.
In medical cases, maltodextrin is being administered widely. MDs are combined with proteins for use of pre-operative feeding and drinks. Administering drinks containing MDs and protein, instead of using the conventional method of preoperative fasting, to patients undergoing major surgery for gastrointestinal malignancies seems to be a practical approach nowadays. But that depends from doctor to doctor.
When it comes to sports, because MDs reduce intestinal distress, it is being used to replace sucrose or glucose in sport drinks. This is relevant since the post-ingestion gastrointestinal distress symptoms are significant performance-limiting factors during running events such as marathons and triathlons exercise.
One benefit of maltodextrin over other forms of simple sugars like glucose, fructose or sucrose is that it is safe for the oral health. Frequent exposure of sugars to teeth is known to cause dental caries. This is a result of the fermentation of the sugars by microorganisms in dental plaque, leading to the formation of organic acids which in turn leads to the demineralization of enamel. Acid in drinks (as common in soft drinks and in juices) enhances this effect further. MDs are less potent in increasing acidity in the oral cavity compared to sucrose.
Resistant MDs are being used as fat replacers due to their ability to form smooth, fat-like gels and their relatively high viscosity. Possible food categories for fat replacement via MDs are low-fat salad dressings, spreads, margarines and butters, mayonnaise, and dairy products. Exchanging fat for MDs, on a w/w basis, will reduce the energy content of the food, as MDs contain less energy/g (4kcal/gm). However, it should be noted, however, that a replacement for fat will not necessarily lead to a reduction of food/energy intake.
IS MALTODEXTRIN WORTH IT?
Now, we need to understand one thing, there is nothing special in maltodextrin as it is same 4kcal/gm as other carb sources. Replacing sugar with maltodextrin is doing no good to anyone. Just like other carb sources, if taken in limited amounts, there is no issue. But, in the amount maltodextrin is added to various sports supplements, specially mass gainers, is nowhere even close to being healthy.
As we saw that maltodextrin is used as a thickener or bulking agent to your supplements. It is added in most mass gainers, because it is quite cheap to procure it in bulk. The GI of maltodextrin, however, is even higher than table sugar (GI is 65), ranging from 95 to 136, which means the spike in blood sugar is even higher than simple sugar.
Though resistant maltodextrin has some benefits for the gut, but that’s not the purpose one takes it for. Because there are many whole foods which can act as excellent prebiotics. So, if a mass gainer is not causing intestinal distress, because of maltodextrin, it nowhere becomes a better option. Maltodextrin is still the same calorie carbohydrate source, and a cheap filler to simply add more calories, with no nutritional value.
On the other hand, the issue with intestinal distress is only till you limit the amount of maltodextrin. High intake of resistant maltodextrin may cause gastrointestinal discomfort due to the gas production. So, if there are studies supporting the use of maltodextrin as a prebiotic, there are other studies condemning it excess use which can cause intestinal disorders.
A 2014 study, suggested that consumption of processed foods containing the polysaccharide maltodextrin contributes to suppression of intestinal anti-microbial defence mechanisms and may be an environmental priming factor for the development of chronic inflammatory disease.
A 2012 research, stated that, the composition and characteristics of the host microbiome are influenced by environmental factors, particularly diet. Polysaccharides added to food as emulsifiers, stabilizers or bulking agents have been linked to bacteria-associated intestinal disorders. The escalating consumption of polysaccharides in Western diets parallels an increased incidence of Crohn’s disease during the latter 20th century.
Maltodextrin enhances E. coli adhesion and suggests a mechanism by which Western diets rich in specific polysaccharides may promote dysbiosis of gut microbes and contribute to disease susceptibility, like autoimmune disorders.
A 2018 meta-analysis study, investigated the evaluation of resistant maltodextrin effects on bowel movements. Researchers found that the intake of resistant maltodextrin significantly increased stool volume and stool frequency compared with placebo intake. Furthermore, resistant maltodextrin intake tended to improve sensation of complete/incomplete evacuation.
In conclusion, the evidence suggests that resistant maltodextrin has a positive effect on bowel movements, contributing to normal bowel function. That’s because of the prebiotic properties of maltodextrin.
However, in a 2019 study, the researchers suggested that, “consumption of the food additive maltodextrin may be a risk factor for the inflammatory bowel disease–prone population, as well as a factor promoting chronic low-grade intestinal inflammation leading to metabolic abnormalities in the general population.”
So, little maltodextrin is not an issue, but your mass gainers, have tons of it, and the calories is still the same, with much higher GI. Therefore, the maltodextrin added in large amounts to your gainers or other supplements are just cheap fillers, with no nutritional value, and the same as sugar.
The only difference is that, it would add bulk to your supplement, and may cause less gastrointestinal distress while consuming these supplements. But in the long run, this less distress can actually lead to serious gut issues.


{kind=link}